


COVID-19 vaccine negative effectiveness in UK booster study

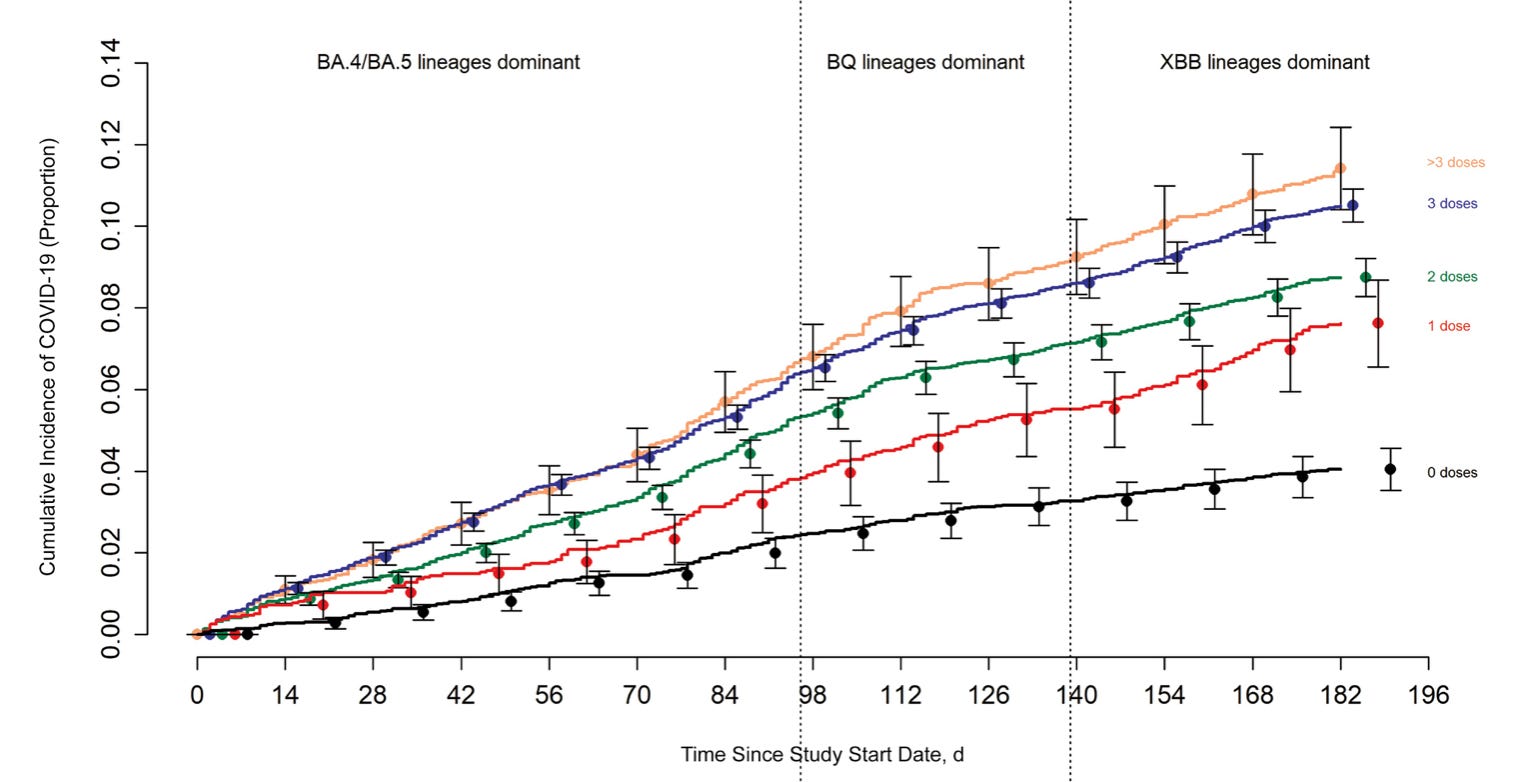
Hot on the heels of my COVID-19 vaccine negative effectiveness article appearing in a major Australian medical journal, a study (Horne et al.) on booster shots involving many millions of Brits found something a little odd: “By 6 months, the cumulative incidence of positive SARS-CoV-2 test was higher in boosted than unboosted individuals.” Source. This not only adds to the increasing evidence of (at least perceived) COVID-19 vaccine negative effectiveness, which is horrifying and needs urgent explanation, but also aligns with the growing evidence that this is dose-dependant, starting from dose 0. Yes, those with 0 doses seem to be at lower risk of getting COVID-19. To up your risk, make sure you’re ‘up to date’ with the jabs. And if you’re one of the morons that for some reason don’t want an increased risk of getting COVID-19, you deserve to be slandered and fired!
Okay then.
Extra: There’s quite a bit more to the UK study. First of all, it aligns a bit with the earlier discussed and related Andrews et al., a big study on UK children (Andrews appears on both papers), with very underwhelming results (no mortality benefit, but clear myocarditis risk). Regarding COVID-19 infections, there was a small decrease in the vaccinated, “although the 20-week risks were similar”. In Horne et al., effectiveness appeared to turn negate for infections at 6 months. What would happen if they looked at the 12 month mark, for both studies? Would it be similar to the other studies showing clear negative effectiveness, even for death, within 12 months? Not to mention more adverse effects can be factored into the risk-benefit analyses, if accuracy and truth is even what they’re striving for (the authors of Andrews et al. had financial ties to government, WHO, the Wellcome Trust, Big Pharma, and that paragon of health, Bill Manboobs Gates). Furthermore, why is the hazard ratio less than 1 for infections in their Table 2 when they clearly stated that there appear to be more infections in the boosted at 6 months? And why does the vaccine in their study apparently have such a dramatic panacea effect on non-COVID deaths, and fractures? They do acknowledge that decreased fractures is surprising, perhaps some confounder is responsible, but would this not also apply to the decreased non-COVID deaths? And could this confounder impact the other outcomes as well, for COVID hospitalisations and death? They did discuss this further, though it was all hypothetical, and I wonder if there is not some confounder/bias/other issue that affected all their results, such as the counting window issues identified by the likes of Peter Doshi and myself in JECP4. I reached out to Andrews for clarification on all this (no response at time of publishing), and on why in Table 3 the best results for the first few months are in days 1-14, when pretty much every other study assumes that it takes 1-2 weeks to build up to ‘full immunity’. I wonder if there is some 1-2 week delay between the jab and ‘full protection’ in Horne et al., which leads to large exaggerations of effectiveness (and even safety), as in almost every other study.
Extra: One of the things that really gets to me about the jabs not being all they were cracked up to be, with these studies and beyond, is that they clearly wanted our children jabbed as well, with the CDC and apparently their allies in the media like CNN recommending “that your children are vaccinated, even if they’ve been infected”. Source. Even though natural immunity is superior, and even though the jab might undo the benefits of natural immunity, and even though COVID vaccination can yield more adverse effects in the previously infected.
This reflects the UKHSA data too. That data is pulled from individual GP Surgeries. Our software system Emis allows analysis of our patient record-level data including time, date and type of vaccination, time of Covid +ve test and death. During the year 2021-22, the UK had a comprehensive testing system for the whole population so we also have decent data on test frequency for vaccinated vs unvaccinated cohorts.
The headlines for my patient population from that time:
- increased doses of the Covid-19 vaccine increased the likelihood of catching Covid afterwards
- the effect became apparent from August 2021 which is just after the first round of vaccinations were completed and during the Summer wave of infection
- testing rates were significantly lower for unvaccinated people. However, the difference in testing rate did not change over time whereas the increasing risk for catching Covid post-vaccination continued to rise for the ever-vaccinated cohort
Anytime I share my findings with fellow UK doctors, they go blank. For many, it's not real unless it's published in a paper. Cognitive dissonance is a helluva drug!
Great work, thanks for the update. I have gone off on a bit of a tangent with my writing as the fraudulent "legal system" is surprisingly fascinating.
I have already realised the entire government works by tricking you in to commercial contracts using implied consent.
When you register to vote you have just signed a contract to be governed. You are trapped.
If you answer the question do you understand with a yes you have just admitted there is a contract. You are trapped.
If you say I will not pay my council tax you have just admitted a contract exists and you have a liability to pay. You are now trapped.
If you answer the question what is your name you have just admitted you are the said “person” (persona or mask) which is a corporation in law. Your name is not you, it is a dead legal fiction. You have just admitted you are responsible for your corporate name and you are now trapped.
Never answer their questions, instead turn the tables on them and start asking (as king) questions.
Questions like why are you guilty according to international law of war crimes, crimes against humanity and genocide?
By paying taxes am I guilty of aiding and abetting war crimes according to international law?
Many more details here; https://truthaddict.substack.com/p/how-to-exit-the-matrix